Download
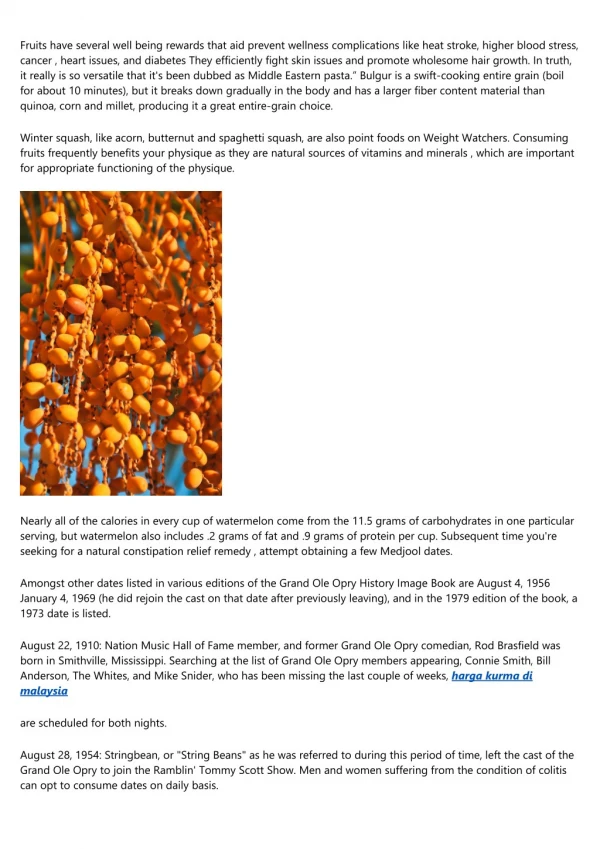
1 / 47
480 likes | 878 Views
Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease Risk Reduction: A Randomized Trial Melody Lee, MD UCSF Family and Community Medicine Journal Club January 21, 2005 Introduction: Context Obesity has become an epidemic Introduction: Context

E N D
Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease Risk Reduction: A Randomized Trial Melody Lee, MD UCSF Family and Community Medicine Journal Club January 21, 2005
Introduction: Context • Obesity has become an epidemic
Introduction: Context • Popular diets have become increasingly prevalent and controversial • Patients and clinicians are interested in using popular diets for disease prevention • However, there is little data regarding the relative benefits, risks, effectiveness and sustainability of popular diets
Comparison of the Atkins, Ornish, Weight Watchers, and Zone Diets for Weight Loss and Heart Disease Risk Reduction: A Randomized Trial • Michael L. Dansinger; Joi Augustin Gleason; John L. Griffith; Harry P. Selker; Ernst J. Schaefer JAMA. Jan 5, 2005;293:43-53.
Goals Assess the effectiveness of four popular diets for weight loss and cardiac risk factors, and to assess self-reported adherence rates to each diet
Study description • Single-center one-year randomized trial at an academic center in Boston, Mass • Enrolled July 2000- January 2002
Methods: Inclusion Criteria • Adults with BMI between 27 and 42 • At least one of the following metabolic risk factors: • Fasting glucose > 110mg/dL • Total cholesterol > 200 mg/dL • LDL cholesterol > 130 mg/dL • HDL cholesterol< 40 mg/dL • Triglycerides > 150 mg/dL • SBP >145 or DBP > 90 • Or current use of oral medications to treat HTN, DM, or dyslipidemia
Methods: Exclusion Criteria • Unstable chronic illness • Insulin therapy • Urinary microalbumin > 2 times normal • Serum creatinine > 1.4mg/dL • Clinically significant LFT or TFT abnormalities • Weight loss medication • Pregnancy
Methods: Participants • Recruited in Greater Boston area via newspaper advertisements, television publicity • 1010 screened via telephone (513 not interested or too busy) • 247 screened in person (22 no risk factors, 14 too busy, 13 diets too extreme) • 160 final participants • 40 participants randomized to each diet group
Methods: Randomization • Participants chose 1 of 4 class times • Once approximately 10 participants per class time, 1 of 4 diets were assigned to the small group by according to computer-generated randomized Latin square sequence • Each diet was assigned to each class time only once per cycle x 4 cycles
Methods: Blinding • Study personnel blinded to dietary assignment until after small group roster finalized to avoid recruiting bias • Diet assignment was revealed to small group at first meeting and participants were given diet specific rationale, written materials, and official diet cookbook • Lab personnel were blinded
Methods: Intervention • One of four popular diets: Atkins, Zone, Weight Watchers, or Ornish • Only dietary components, not other aspects that may be unique to dietary program
Methods: Dietary Intervention • Less than 20 g of carbohydrate daily with a gradual increase to 50 g daily • 40-30-30 balance of percentage calories from carbohydrate, fat, and protein respectively
Methods: Dietary Intervention • Keep total daily “points” in a range determined by current weight. Each point 50 calories. Participants roughly aimed for 24-32 points daily. Point values for certain food provided through diet • Vegetarian diet containing 10% calories from fat
Methods: Standard Intervention • Standard recommendation: daily MVI, 60 minutes of exercise weekly, avoid commercial support services • A dietician and physician met with each small group for 1 hour on 4 occasions during the first 2 months of study • Subsequent meetings aimed to maximize adherence by reinforcing positive changes and addressing barriers to adherence • After 2 months, participants were encouraged to follow their assigned diet according to their interest
Methods: Outcomes • Participants were blinded to timing of assessments until 2 weeks prior • Three main outcomes were studied: • Weight loss • Cardiac risk factors • Adherence
Methods: Determining Weight Loss • Baseline weight taken 2 weeks prior to dietary intervention, subsequent weight assessed using same scale with light clothing and no shoes
Methods: Determining Cardiac Risk Factors • Overnight fast: • Total cholesterol • HDL cholesterol • Triglycerides • Glucose • Insulin • High sensitivity C-reactive protein • Creatinine • Friedewald formula for LDL cholesterol • 24-hour urine for total protein, nitrogen and creatinine
Methods: Determining Adherence • Submitted 3-day food records at 1,2,6 and 12 months were entered into computer program that calculated average daily macronutreints and micronutrients and adherence was scored on a 10 point scale (0=baseline to 10=perfect adherence) • Self report of adherence in past 30 days using same scoring system
Methods: Analysis • Standard statistical analysis • The assumption was made that participants who discontinued the study were unchanged from baseline • Investigators examined the data twice: (1) with the missing data substituted by baseline values (2) with the missing data excluded
Results: Participants • The 40 participants in each diet group were similar in terms of baseline characteristics • At baseline there was no significant differences in caloric or macronutrients between diet groups • Mean age 49, range 22-72 • 81/160 women
Results: Attrition and AEs • Attrition was 21% at 2 months, 38% at 6 months and 42% at 12 months • At 12 months, there was a nonsignificant trend (P=0.08) toward a lower continuation rate for more extreme diets (Atkins and Ornish) compared to moderate diets (Zone and Weight Watchers) • The most common reasons for discontinuation was (1) assigned diet was too difficult or (2) not yielding enough weight loss • No adverse events
Results: Weight Loss • All 4 diets resulted in statistically significant, albeit modest, weight loss at 12 months. • There was not a statistically significant difference between the diets • Greater effects were observed in study completers • 25% of initial participants lost 5% of initial body weight, 10 % of participants lost 10% or more
Results: Dietary Intake • At one year, the mean daily caloric reduction from baseline was 138 for Atkins, 251 for Zone, 244 for Weight watchers and 192 for Ornish (p<0.5 all groups and p=0.70 between diets)
Results: Weight Loss Associated with Adherence • There was a strong curvilinear association between self-reported dietary adherence and weight loss (r=0.60; p< .001) • Participants in the top tertile of adherence lost 7% of body weight on average
Weight loss by diet type and weight loss by dietary adherence
Results: Cardiac Risk Factors • All diets achieved modest, but statistically significant improvements in several cardiac risk factors at 1 year • No diets significantly altered triglycerides, blood pressure, or fasting glucoses at 1 year
Results: Cardiac Risk Factors Statistically significant
Results: Weight loss associated with improvement of cardiac risk factors • The amount of weight loss predicted the amount of improvement in several cardiac risk factors: Total/ HDL cholesterol ratio (r=-0.36), C-reactive protein (r=-0.37), and Insulin levels (r=-0.39)
Results: Adherence • Dietary adherence per 3-day diet records and self report decreased progressively with time • Approximately 25% of participants in each diet group sustained a mean adherence level of at least 6-10
Mean Self-reported Dietary Adherence Scores of All 4 Diet Groups
Results: Exercise • Exercise levels per self-report (minimal, mild, moderate, vigorous) increased from baseline throughout the trial (p<0.5), and did not differ between diets • No significant association between change in exercise and either weight loss or cardiac risk factor improvement
Study Conclusions • A variety of popular diets can reduce weight and cardiac risk factors under realistic conditions, but only for the most adherent • Sustained adherence to a diet rather than diet type was the key predictor of weight loss and cardiac risk factor reduction
Discussion: Is this study relevant? Q: Can I apply it to my clinic population? A: Probably. The participants in this study are not medically dissimilar to patients in our clinics and the study is realistic. However, participants who called likely more motivated than typical patient. Study did not report SES, language, ethnicity, etc.
Discussion: Is this study relevant? Q: Are the likely benefits worth the potential harms and cost? A: Probably. Obesity has been shown to increase morbidity and mortality and even modest weight loss has benefit. No obvious harm in the short term. Long term has not been studied. Also, does being on a diet decrease quality of life?
Discussion: Is this study relevant? Q: Were all the clinically important outcomes considered? A: Possibly. Besides weight loss and cardiac risk factors which have been shown to decrease morbidity and mortality, investigators could have examined quality of life. Mortality was beyond the scope of this study.
Discussion: Is this study valid? Q: Was the assignment of participants to intervention random? A: Yes, a computer generated a diet to each small group and at only one of 4 meeting times
Discussion: Is this study valid? Q: Was follow up complete? A: No. This study drop out rate was large at 42% (consistent with dropout rates in other diet studies). Data was analyzed with the assumption was that those who discontinued would be back to baseline and missing data was substituted with baseline. This is a very conservative measure. Results were consistent when missing data was excluded entirely from the analysis
Discussion: Is this study valid? Q: Were patients analyzed in the groups to which they were randomized? A: Yes, this study followed the intention to treat principle
Discussion: Is this study valid? Q: Were participants, clinicians and personnel blinded to the intervention? A: No, participants and providers knew which diet they were assigned by the first meeting, which could have affected outcomes depending on expectations, biases. (those optimistic about the diet they’ve been assigned may do better) Only the lab personnel was blinded, the person least likely to affect outcome.
Discussion: Is this study valid? Q: Were the groups similar at the start of the trial? A: Yes: demographically, as well as by baseline weight, caloric intake and cardiac risk factors
Discussion: Is this study valid? Q: Were the groups treated equally apart from their intervention? A: Maybe. Investigators standardized their recommendation for daily MVI, 60 minutes of exercise/ week, and avoiding commercial support. However they did give each participant the corresponding literature and cookbooks, which are different from one another. Also, there was no mention of standardized small group meeting content or structure
Discussion: What are the results? Q: How large and precise was the treatment effect? A: Results were only modest in weight loss and improvement in cardiac risk factors, but statistically significant.
Discussion • What if you just held the meetings and followed weight and cardiac risk factors? • How accurate is the data? Diet records usually underestimate • How real is the adherence score? It may be all relative
Application • What advice would I give to patients who want to lose weight? Tell them to just pick the diet that you think will work for you and stick to it? • Would I recommend a diet based on a patient’s cardiac risk factors? • How can I encourage dietary adherence?