Download
1 / 2
20 likes | 397 Views
A B C D E Early Assessment of Therapeutic Response in Hepatocellular Carcinoma Treated with Percutaneous Radio-frequency Ablation: A Comparison of Multiphase Helical CT and Power Doppler US with a Microbubble Contrast Agent

E N D
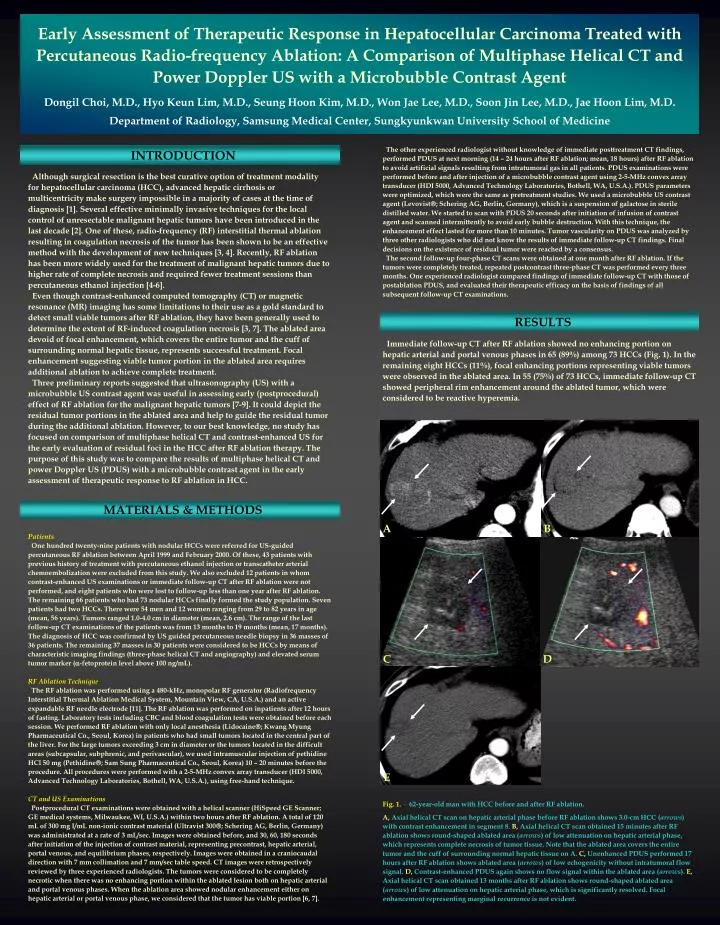
A B C D E Early Assessment of Therapeutic Response in Hepatocellular Carcinoma Treated with Percutaneous Radio-frequency Ablation: A Comparison of Multiphase Helical CT and Power Doppler US with a Microbubble Contrast Agent Dongil Choi, M.D., Hyo Keun Lim, M.D., Seung Hoon Kim, M.D., Won Jae Lee, M.D., Soon Jin Lee, M.D., Jae Hoon Lim, M.D. Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine The other experienced radiologist without knowledge of immediate posttreatment CT findings, performed PDUS at next morning (14 – 24 hours after RF ablation; mean, 18 hours) after RF ablation to avoid artificial signals resulting from intratumoral gas in all patients. PDUS examinations were performed before and after injection of a microbubble contrast agent using 2-5-MHz convex array transducer (HDI 5000, Advanced Technology Laboratories, Bothell, WA, U.S.A.). PDUS parameters were optimized, which were the same as pretreatment studies. We used a microbubble US contrast agent (Levovist; Schering AG, Berlin, Germany), which is a suspension of galactose in sterile distilled water. We started to scan with PDUS 20 seconds after initiation of infusion of contrast agent and scanned intermittently to avoid early bubble destruction. With this technique, the enhancement effect lasted for more than 10 minutes. Tumor vascularity on PDUS was analyzed by three other radiologists who did not know the results of immediate follow-up CT findings. Final decisions on the existence of residual tumor were reached by a consensus. The second follow-up four-phase CT scans were obtained at one month after RF ablation. If the tumors were completely treated, repeated postcontrast three-phase CT was performed every three months. One experienced radiologist compared findings of immediate follow-up CT with those of postablation PDUS, and evaluated their therapeutic efficacy on the basis of findings of all subsequent follow-up CT examinations. INTRODUCTION Although surgical resection is the best curative option of treatment modality for hepatocellular carcinoma (HCC), advanced hepatic cirrhosis or multicentricity make surgery impossible in a majority of cases at the time of diagnosis [1]. Several effective minimally invasive techniques for the local control of unresectable malignant hepatic tumors have been introduced in the last decade [2]. One of these, radio-frequency (RF) interstitial thermal ablation resulting in coagulation necrosis of the tumor has been shown to be an effective method with the development of new techniques [3, 4]. Recently, RF ablation has been more widely used for the treatment of malignant hepatic tumors due to higher rate of complete necrosis and required fewer treatment sessions than percutaneous ethanol injection [4-6]. Even though contrast-enhanced computed tomography (CT) or magnetic resonance (MR) imaging has some limitations to their use as a gold standard to detect small viable tumors after RF ablation, they have been generally used to determine the extent of RF-induced coagulation necrosis [3, 7]. The ablated area devoid of focal enhancement, which covers the entire tumor and the cuff of surrounding normal hepatic tissue, represents successful treatment. Focal enhancement suggesting viable tumor portion in the ablated area requires additional ablation to achieve complete treatment. Three preliminary reports suggested that ultrasonography (US) with a microbubble US contrast agent was useful in assessing early (postprocedural) effect of RF ablation for the malignant hepatic tumors [7-9]. It could depict the residual tumor portions in the ablated area and help to guide the residual tumor during the additional ablation. However, to our best knowledge, no study has focused on comparison of multiphase helical CT and contrast-enhanced US for the early evaluation of residual foci in the HCC after RF ablation therapy. The purpose of this study was to compare the results of multiphase helical CT and power Doppler US (PDUS) with a microbubble contrast agent in the earlyassessment of therapeutic response to RF ablation in HCC. RESULTS Immediate follow-up CT after RF ablation showed no enhancing portion on hepatic arterial and portal venous phases in 65 (89%) among 73 HCCs (Fig. 1). In the remaining eight HCCs (11%), focal enhancing portions representing viable tumors were observed in the ablated area. In 55 (75%) of 73 HCCs, immediate follow-up CT showed peripheral rim enhancement around the ablated tumor, which were considered to be reactive hyperemia. MATERIALS & METHODS Patients One hundred twenty-nine patients with nodular HCCs were referred for US-guided percutaneous RF ablation between April 1999 and February 2000. Of these, 43 patients with previous history of treatment with percutaneous ethanol injection or transcatheter arterial chemoembolization were excluded from this study. We also excluded 12 patients in whom contrast-enhanced US examinations or immediate follow-up CT after RF ablation were not performed, and eight patients who were lost to follow-up less than one year after RF ablation. The remaining 66 patients who had 73 nodular HCCs finally formed the study population. Seven patients had two HCCs. There were 54 men and 12 women ranging from 29 to 82 years in age (mean, 56 years). Tumors ranged 1.0-4.0 cm in diameter (mean, 2.6 cm). The range of the last follow-up CT examinations of the patients was from 13 months to 19 months (mean, 17 months). The diagnosis of HCC was confirmed by US guided percutaneous needle biopsy in 36 masses of 36 patients. The remaining 37 masses in 30 patients were considered to be HCCs by means of characteristic imaging findings (three-phase helical CT and angiography) and elevated serum tumor marker (-fetoprotein level above 100 ng/mL). RF Ablation Technique The RF ablation was performed using a 480-kHz, monopolar RF generator (Radiofrequency Interstitial Thermal Ablation Medical System, Mountain View, CA, U.S.A.) and an active expandable RF needle electrode [11]. The RF ablation was performed on inpatients after 12 hours of fasting. Laboratory tests including CBC and blood coagulation tests were obtained before each session. We performed RF ablation with only local anesthesia (Lidocaine; Kwang Myung Pharmaceutical Co., Seoul, Korea) in patients who had small tumors located in the central part of the liver. For the large tumors exceeding 3 cm in diameter or the tumors located in the difficult areas (subcapsular, subphrenic, and perivascular), we used intramuscular injection of pethidine HCl 50 mg (Pethidine; Sam Sung Pharmaceutical Co., Seoul, Korea) 10 – 20 minutes before the procedure. All procedures were performed with a 2-5-MHz convex array transducer (HDI 5000, Advanced Technology Laboratories, Bothell, WA, U.S.A.), using free-hand technique. CT and US Examinations Postprocedural CT examinations were obtained with a helical scanner (HiSpeed GE Scanner; GE medical systems, Milwaukee, WI, U.S.A.) within two hours after RF ablation. A total of 120 mL of 300 mg I/mL non-ionic contrast material (Ultravist 300; Schering AG, Berlin, Germany) was administrated at a rate of 3 mL/sec. Images were obtained before, and 30, 60, 180 seconds after initiation of the injection of contrast material, representing precontrast, hepatic arterial, portal venous, and equilibrium phases, respectively. Images were obtained in a craniocaudal direction with 7 mm collimation and 7 mm/sec table speed. CT images were retrospectively reviewed by three experienced radiologists. The tumors were considered to be completely necrotic when there was no enhancing portion within the ablated lesion both on hepatic arterial and portal venous phases. When the ablation area showed nodular enhancement either on hepatic arterial or portal venous phase, we considered that the tumor has viable portion [6, 7]. Fig. 1.__ 62-year-old man with HCC before and after RF ablation. A, Axial helical CT scan on hepatic arterial phase before RF ablation shows 3.0-cm HCC (arrows) with contrast enhancement in segment 8. B, Axial helical CT scan obtained 15 minutes after RF ablation shows round-shaped ablated area (arrows) of low attenuation on hepatic arterial phase, which represents complete necrosis of tumor tissue. Note that the ablated area covers the entire tumor and the cuff of surrounding normal hepatic tissue on A. C, Unenhanced PDUS performed 17 hours after RF ablation shows ablated area (arrows) of low echogenicity without intratumoral flow signal. D, Contrast-enhanced PDUS again shows no flow signal within the ablated area (arrows). E, Axial helical CT scan obtained 13 months after RF ablation shows round-shaped ablated area (arrows) of low attenuation on hepatic arterial phase, which is significantly resolved. Focal enhancement representing marginal recurrence is not evident.
C D A B E C D F G E A B Unenhanced PDUS after RF ablation showed no flow signals within the tumor in all 73 HCCs. However, in eight HCCs (11%), focal intratumoral flow signals newly appeared on contrast-enhanced PDUS (Fig. 2). These eight tumors with intratumoral flow signals had enhancing portions on immediate follow-up CT (Fig. 2). The areas of the tumors where power Doppler signals were found were well correlated with the enhancing portions at CT in all eight tumors. Therefore, diagnostic agreement between contrast-enhanced US and immediate follow-up CT was achieved in 100%. Contrast-enhanced PDUS after RF ablation showed increased flow signals representing reactive hyperemia around the ablated areas in 34% (25 of 73 HCCs). Fig. 3.__ 43-year-old man with HCC before and after RF ablation. A, Axial helical CT scan on hepatic arterial phase before RF ablation shows 4.0-cm HCC (arrows) with contrast enhancement in segment 5. B, Axial helical CT scan obtained 25 minutes after RF ablation shows round-shaped ablated area (arrows) of low attenuation on hepatic arterial phase, which represents complete necrosis of tumor tissue. Note that the ablated area is slightly larger than initial tumor on A. Also seen is semicircular peripheral reactive hyperemia (arrowheads). C, Unenhanced PDUS performed 16 hours after RF ablation shows ablated area (arrows) of mixed echogenicity without intratumoral flow signal. D, Contrast-enhanced PDUS again shows no flow signal within the ablated area (arrows). Increased flow signals indicating reactive hyperemia are seen around the ablated area. E, Axial helical CT scan on hepatic arterial phase obtained 4 months after RF ablation shows that most ablated area (arrows) is of low attenuation, but a subtle focal enhancing portion (arrowhead) is noted in the posterior side of the ablated area. The nodular enhancement represents viable tumor portion. F, T1-weighted fast multiplanar spoiled gradient echo (TR200/TE4.2/flip angle 90˚) image shows the ablated area (arrows) with high signal intensity, probably representing coagulation necrosis. G, T1-weighted fast multiplanar spoiled gradient echo image obtained 1-minute after administration of gadolinium shows a new nodular lesion (arrowhead) with high signal intensity. This nodular enhancement represents viable tumor, which is well correlated with that at CT on E. Fig. 2.__ 46-year-old man with HCC before and after RF ablation. A, Axial helical CT scan on hepatic arterial phase before RF ablation shows 3.8- cm HCC (arrows) with contrast enhancement in segment 5. B, Axial helical CT scan on hepatic arterial phase obtained 20 minutes after RF ablation shows that most ablated area is of low attenuation, but a focal enhancing portion (yellow arrowhead) is noted in the right anterior side of the ablated area (arrows) with semicircular peripheral reactive hyperemia (black arrowheads). The nodular enhancement represents viable tumor portion. C, Unenhanced PDUS performed 19 hours after RF ablation shows ablated area (arrows) of low echogenicity without flow signal. D, Contrast-enhanced PDUS shows focal peripheral flow signals (yellow arrowhead) within the ablated area (arrows), which represent residual tumor vessels. Also seen is reactive hyperemia (white arrowheads). The residual tumor was treated with additional RF ablation on the same day. E, Axial helical CT scan obtained 1 month after additional ablation shows oval-shaped ablated area (arrows) of low attenuation on hepatic arterial phase, which represents complete necrosis of tumor tissue. DISCUSSION We believe that contrast-enhanced US enables a practical early assessment of HCCs treated with RF ablation. It satisfies to determine the clinical decision for additional ablation and helps to guide the residual foci of tumors. We can adopt the strategy of performing contrast-enhanced US scans in the next morning after RF ablation. If vessels are found in the ablated tumor on contrast-enhanced US, an additional RF ablation therapy is performed with targeting intratumoral vessels. In our opinion, immediate follow-up CT scans are not necessary. Considering possibility of CT and subsequent US for additional RF ablation, immediate follow-up CT scans can be expensive and too much. Although postprocedural PDUS with a microbubble contrast agent may depict many residual tumors in HCCs treated with percutaneous RF ablation, it can not completely prevent marginal recurrence. However, newer development of US contrast agent and US technology such as harmonic imaging can improve the ability to detect smaller viable tumor in the ablated area [10]. In conclusion, compared with the findings of immediate follow-up CT, the results of contrast-enhanced PDUS correlated well for the early detection of residual tumor in HCCs treated with RF ablation. Both techniques, however, had a limitation in predicting the local re-growth in the treated lesion. Among the 65 ablated HCCs without residual tumor at both immediate contrast-enhanced CT and PDUS after the initial RF ablation, ten (15%) had CT findings of marginal recurrence at 4-month (n=5) (Fig. 3), at 7-month (n = 4), and at 10-month follow-up CT (n = 1), respectively. These findings of marginal recurrence could not be retrospectively observed at immediate follow-up CT. Among eight patients with residual nodular enhancement at CT and intratumoral flow signals on contrast-enhanced PDUS, seven were treated with additional RF ablation. The remaining one patient was treated with transcatheter arterial chemoembolization because the residual tumor was located in difficult area -just below the cardiac base. After RF ablation, we observed no major complication and five minor complications (four cases of minor perihepatic hemorrhage and one small pneumothorax), which disappeared spontaneously with no specific treatment. REFERENCES 1. Schafer DF, Sorrell MF. Hepatocelluar carcinoma. Lancet1999; 353:1253-1257 2. DoddGD III, Soulen MC, Kane RA, et al. Minimally invasive treatment of malignant hepatic tumors: at the threshold of a major breakthrough. Radiographics2000; 20: 9-27 3. Livraghi T, Goldberg SN, Monti F, et al. Saline-enhanced radio-frequency tissue ablation in the treatment of liver metastases. Radiology1997; 202:205-210 4. Rossi S, Buscarini E, Garbagnati F, et al. Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR1998; 170:1015-1022 5. Livraghi T, Goldberg SN, Lazzarni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology1999; 210:655-661 6. Lim HK. Radiofrequency thermal ablation of hepatocellular carcinomas. Korean J Radiol2000; 1:175-184 7. Solbiati L, Goldberg SN, , Ierace T, Dellanoce M, Livraghi T, Gazelle GS. Radio-frequency ablation of hepatic metastases: postprocedural assessment with a US microbubble contrast agent – early experience. Radiology1999; 211:643-649 8. Goldberg SN, Walovitch RC, Straub JA, Shore MT, Gazelle GS. Radio-frequency-induced coagulation necrosis in rabbits: immediate detection at us with a synthetic microsphere contrast agent. Radiology1999; 213: 438-444 9. Choi D, Lim HK, Kim SH, et al. Hepatocellular carcinoma treated with percutaneous radio-frequency ablation: usefulness of power Doppler US with a microbubble contrast agent in evaluating therapeutic response-preliminary results. Radiology2000; 217: 558-563 10. Frinking PJ, Bouakaz A, Kirkhorn J, Ten Cate FJ, de Jong N. Ultrasound contrast imaging: current and new potential methods. Ultrasound Med Biol2000; 26:965-975






