Download

1 / 17
170 likes | 568 Views
Transition of Care in a Community Hospital. Sarah Vickey, PharmD, BCACP Ephraim McDowell Regional Medical Center. Disclosure . I have nothing to disclose. Educational Need/Practice Gap.

E N D
Transition of Care in a Community Hospital Sarah Vickey, PharmD, BCACP Ephraim McDowell Regional Medical Center
Disclosure • I have nothing to disclose
Educational Need/Practice Gap • Thirty day readmission rates for hospitals are under surveillance because of potential reimbursement reductions • Hospital specific programs are being developed and employed by various institutions to help reduce readmission rates and improve patient outcomes
Objectives • Explain WHY we started our program at Ephraim McDowell Regional Medical Center (EMRMC) • Review the functionality of the transition of care program at EMRMC • Explain the benefits of the EMRMC transition of care program
Test your knowledge Which of the following disease states is NOT reviewed for readmission rates by CMS? • Acute Myocardial Infarction • Pneumonia • Acute Kidney Disease • Heart Failure
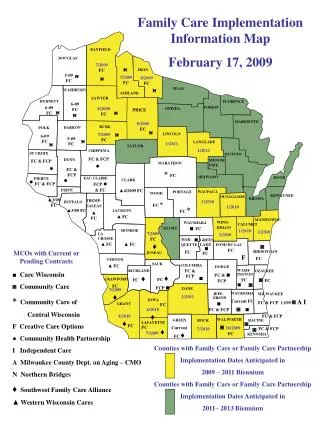
Background • Ephraim McDowell Regional Medical Center is a 222 bed hospital serving 5 counties in rural KY • Our TOC program launched (2013) in response to regulatory reimbursement changes • Potential loss of $900,000 in 2015 if readmission rates sustained • EMRMC chose to initially prioritize CHF and COPD • 2 highest readmission rates at EMRMC (2013) • PNA and AMI were subsequently added • Multi-disciplinary approach • Case Management • Pharmacy (both inpatient and outpatient) • Respiratory • Dietary
Program Outline • A specific department is responsible for screening admitted patients for its delegated disease state(s): • Case management/Inpatient Pharmacy - CHF; PNA • Respiratory - COPD • Cath Lab - AMI • Program offered to patients with a new, qualifying diagnosis or multiple admissions • Amenable patients are given disease state education • May occur at any point during hospital stay • Written form • Video via Xplain app (iPad) • Upon hospital discharge, prescribers have access to protocols which aid drug selection for each corresponding disease state; these meds are available to patients at NO charge • EMRMC is a DSH hospital - enables us to offer inexpensive drugs at NO charge • Each protocol is updated with guideline updates • All programs offer a 30 days supply (except PNA)
Program • In addition to medications, patients are provided: • Water bottle, Mrs. Dash samples (HF), Crystal Light Samples (COPD) • Sample recipes • 2 week pass to EMRMC Wellness Center • Post discharge patients are telephoned weekly by a team member • Each disease state has a built-in intervention in our EMR system to ensure consistent questioning • Calls are made on post-discharge days: 7, 14, 21, 28 • PNA patients are followed for 14 days • Purpose of each telephone call is to ensure: • Patient has been to their PCP within 7 days post discharge • Patient is not having any unwanted/unusual side effects • Patient affordability and adherence to refills
Example of Questions for Day 7 follow up for COPD
Results TARGET: < 1.2
Future • EMRMC would like to continue to follow these 4 disease states and possibly integrate Stroke and Hip or Knee replacement • We are already meeting our goal for YTD on these disease states; therefore there is less urgency to implement them • Improve screening processes to identify and improve upon missed opportunities
Review Question What is the goal for readmission rate? • 1.5 • 1.2 • 1 • 0.9